Bowel preparation plays a key role in your child having a successful paediatric colonoscopy
 residue coating the lining of the large intestine making it very hard to assess properly")
 residue coating the lining of the large intestine making it very hard to assess properly")
The days before a paediatric colonoscopy is when you and your child can really have a positive impact on optimising the appearance of the bowel lining during the colonoscopy.
Why does your child need a colonoscopy
First let's recap how we got to the point of your child needing a colonoscopy.
Your child has been having tummy troubles for some time. In some it may be prolonged diarrhoea (usually for longer than the usual 2-3 weeks that can happen with an infection) and can be accompanied by abdominal pain, weight loss and tiredness.
In some children there may be visible blood or mucus seen with the looser stools.
You may be concerned that there symptoms are similar to those of a close relative with a bowel condition.
Your doctor has performed some non-invasive investigations, such as blood tests and stool (faeces or poo) tests, including a faecal calprotectin. This is a protein released by white cells called neutrophils, that accumulate in areas of inflammation.
The results have come back and shown the possibility of significant gut inflammation. They don't make a diagnosis, for this the next step is that they need a paediatric colonoscopy to investigate things further.
You've seen a paediatric gastroenterologist about this. They have assessed your child and their situation, reviewed the tests performed so far. They recommend proceeding with endoscopy, in this case including a paediatric colonoscopy. They have booked your child in for the procedure.
What happens in the colon
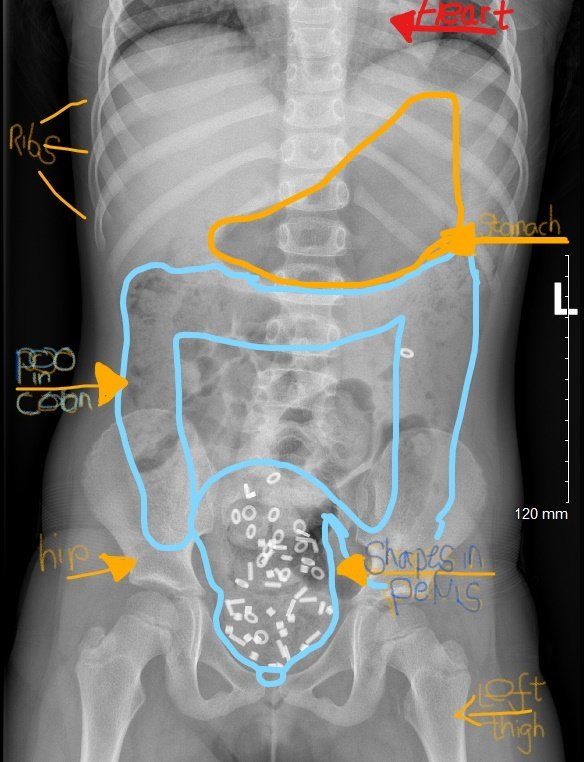
You may recall that the digestive system is, in very simple terms, essentially a long tube that stretches from the mouth, through the oesophagus and stomach and into the small and then large intestines and empties via the rectum. Each area plays a different role in the digestive process.
Nutrients are absorbed throughout the small intestine. The colon (or large intestine) is where the leftover waste matter is processed and turned into what we recognise as poo (stool or faeces).
How much poo is in the colon, and what consistency it is, depends on the type of food we eat, how much we eat, how fast or slow your bowel moves the contents along, how much water is absorbed as the residue travels along the colon amongst other factors including any medications being used.
What happens during a colonoscopy
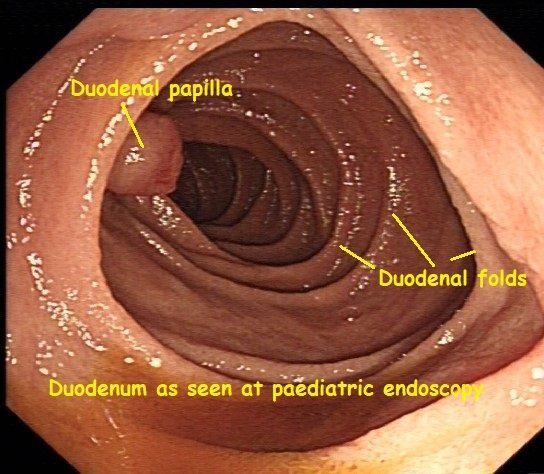
During any colonoscopy, whether in an adult or a child, the adult or paediatric gastroenterologist or endoscopist, inserts a long flexible floppy tube that contains intricate technology within it, and that has a light and video camera at one end, into the large intestine via the rectum (back passage). The camera's images are transmitted to a large high definition monitor that is directly opposite the endoscopist.
Any paediatric endsocopist or gastroenterologist hopes that the patient has good bowel preparation. They want to get as clear a view of the lining (also known as the mucosa) of the colon as possible. This is so that they can observe and document, with photographs, any areas that look abnormal. They can also take samples of tissue, known as biopsies, from those areas for more detailed analysis.
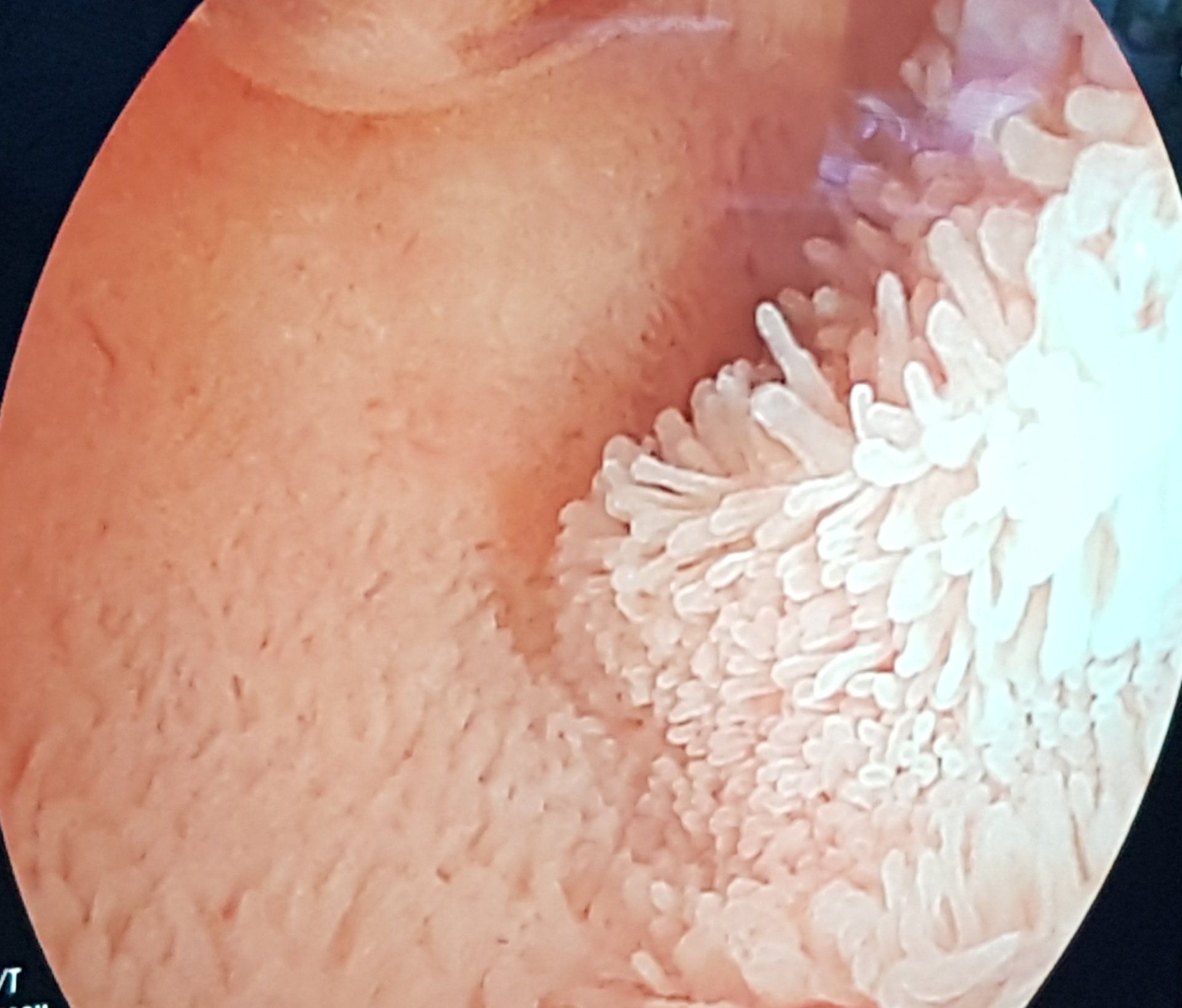
The picture here shows a very heavy amount of poo residue obscuring the view of the lining of the colon. This makes it very hard for the specialist to distinguish any areas of linng whether normal or abnormal at all.
This prolongs the procedure substantially. In children, who have endoscopy performed whilst they are under general anaesthetic, this means more time spent under the influence of general anaesthetic. It also adds another layer of risk should any complication, for example perforation, although rare, occur.
Can't the doctor just get rid of the poo?
Whilst it is possible to use a water jet wash to clear some of the residue away (hover over the image with your mouse to see what I mean), with such a heavy amount of poo about, it adds a lot of time of the procedure. Poo residue also increases the risk of missing any pathology and can also mean cutting the procedure short, so an incomplete procedure.
What can parents and children do ahead of any colonoscopy?
You have a vital role. The time spent on preparing one's child or teen for a colonoscopy is well worth it, in terms of:
- safety
- getting the most information out of the procedure as possible
- minimising the time spent asleep with general anaesthetic.
The days before a colonoscopy are crucial as they are when you and your child can have a very positive impact on bowel preparation, that is, optimising the appearance of the bowel lining during the colonoscopy.
What is bowel preparation
This is the important act of getting the colon ready for procedures such as paediatric colonoscopy, so that the colon is effectively cleansed and has minimal poo residue within it during the procedure.
There are two phases to bowel preparation:
1st phase - Dietary changes
Your doctor and their team will give you specific instructions about modifying your child's diet in the 2-3 days before the procedure.
The advice is to:
- avoid eating high fibre foods
- then switch to diet that has only low residue foods.
This is all with the aim of having far less poo residue left in the colon before the procedure than one would have when on a normal fibre and normal residue diet.
Your team will provide you with a list of suitable foods so that you can prepare ahead of the procedure. It is important to prepare your child to understand that their diet will be different for a few days, to make it easier to see inside the colon properly.
2nd phase - Strong laxatives the day before colonoscopy
The day before a paediatric colonoscopy, your child or teen will need to drink some very strong laxatives. These aren't available over the counter. They are often prescribed by the doctor you met in a clinic, sent out by the endoscopy unit where the procedure will take place, or a prescription may be posted to you.
In the UK there are a variety of laxatives used. In children we commonly use laxatives that increase the water content of the stools making them a lot looser. They also cause the bowel to contract to push the poo out. Different brands exist such as Picolax, Moviprep etc. Sometimes combinations of common laxatives are used.
They may be specially adapted to lower doses for smaller children.
It is important to closely follow the instructions sent to you including the amount to give your child and also the timing of when to give the laxatives.
Often 2 doses are given several hours apart on the day before the colonoscopy.
Over the course of the 24 hours before the procedure your child will experience the need to urgently get to the toilet, and the stools may become very watery, to the point where it can be difficult to keep control of the bowels. Sometimes accidents or leaks can happen. This is not your child's fault.
To make the experience as comfortable as possible, it is best to stay off school, nursery or college the day before the colonoscopy whilst taking these laxatives.
Top tips for bowel preparation in children having a colonoscopy
Prepare your child ahead of any procedures - talk them through what is going to happen using age appropriate terms. Your doctor will often have done this in clinic and can provide age appropriate resources to read through or links to videos to watch.
Plenty are also available on the web.
Knowing what is ahead is usually better than springing a surprise and not being prepped.
Shop ahead for fun low residue foods
Have a good look at the list of allowed low residue foods sent to you by your doctor. Discuss these with your child and see what they would like from them. Have them all ready so that you're all set for the days before the procedure.
Let school and your work know
Tell your child's school that they will miss school the day before and the day of the colonoscopy procedure. Let your family and work colleagues know that you will be needed by your child on those days.
The day before the colonoscopy and taking the Bowel prep laxatives
Make sure your prescription is available at your local pharmacy and picked up well ahead of the procedure - avoid any last minute panic hunting for a pharmacy that supplies the medicine. Have this all ready at home days before the procedure.
Stay at home the day before procedure - so much more comfortable for all involved
Follow the instructions on how to make the prep medicine and use these tips when using it
- Let it get cold- the colder the better. Often these medicines generate heat when made up
- Flavour it with an allowable and child-friendly taste - a cordial for example
- Use a straw
- Drink plenty of water - especially in younger children, but in all ages it is important to keep your child hydrated
- Plan to be close to a toilet. Few things are more distressing than getting caught short when out and about. Having a familiar bathroom and toilet nearby makes for a far more pleasant experience. One of the benefits of being at home for this if age allows.
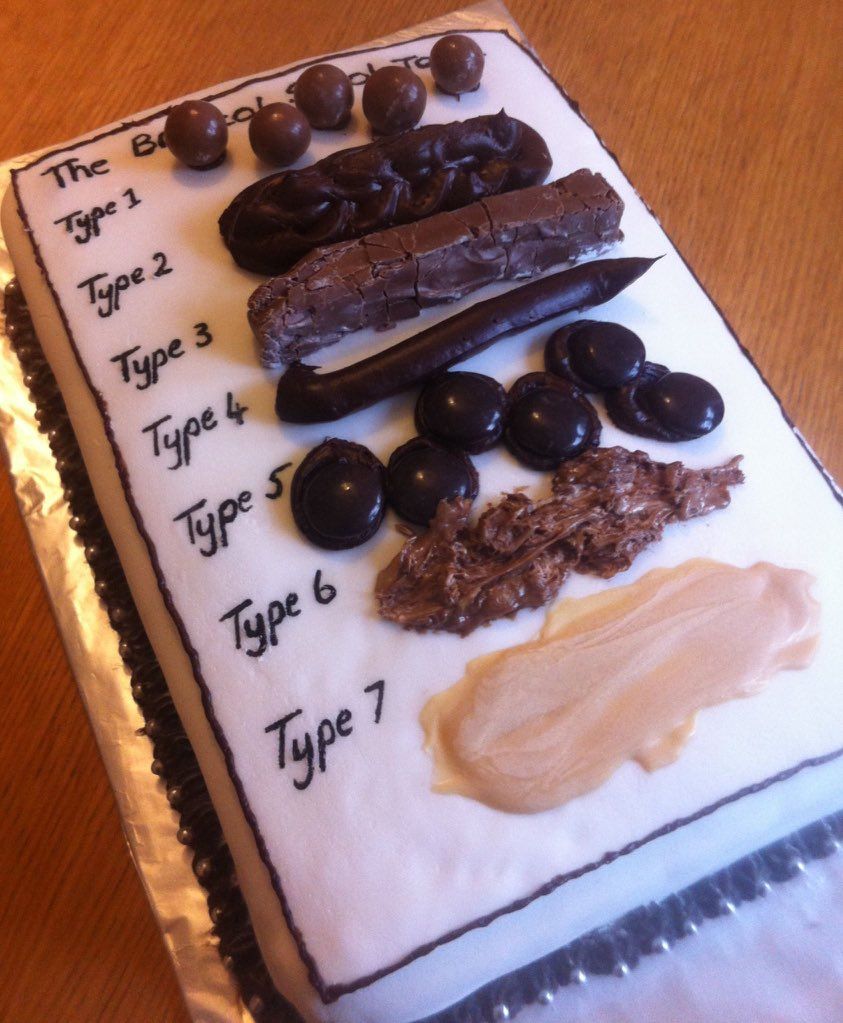
- You or your child should have a good look at what consistency of poo is coming out - the nurses or doctors will want to know if the bowel preparation has worked well enough. Ideally the poo should be very watery (almost like wee -or type 7 on the Bristol stool chart) with just bits in it. If it hasn't turned that watery or there is a doubt, the team may prescribe a rectal laxative called an enema to get a final clear out of any residue so that the colon is cleansed thoroughly ahead of any colonoscopy
- Follow the fasting instructions that your team has sent you. It is important when having an anaesthetic that these are followed closely to minimise any risk of stomach contents coming up and then going down the windpipe whilst asleep (known as aspiration)
If you're in any doubt or have any questions about any of this process ahead of your child's colonoscopy, then please ask your doctor or the endoscopy team.
Remember that we all want to get the most information, in the safest possible way, from any paediatric colonoscopy. So getting bowel preparation right is a crucial role that you and your child have.
For more information about tests including paediatric endoscopy click here.
If you are concerned about tummy troubles that your child has, and you think they need an evaluation with an experienced paediatric gastroenterologist, then please do be in touch by emailing us
Wishing you and your child all the best with getting ready for their colonoscopy.
Dr Crespi
Much Ado about Poo